NICL Laboratories MDRO & Antimicrobial Susceptibility Test Report
NICL MASTRsm is a compilation of one whole year of NICL Laboratories antimicrobial susceptibility testing. The data is from hundreds of facilities throughout the greater Chicagoland area, representing a population of tens of thousands beds. Our service area makes us uniquelyprepared for tracking MDRO emergence, as well as for providing a report of this nature. For this reason, we have made this annual report available not only to our clients, but to any other members of the medical community and the general public who may benefit from this information. Read more
NICL Laboratories is introducing new technology to Microbiology in May 2022. The new technology is MALDI-TOF or matrix assisted laser desorption/ionization-time of flight, and it will be performed on the Bruker Sirius ONE MALDI Biotyper® CA System.
This technology uses high mass spectrometric resolution to rapidly and accurately identify microorganisms in a matter of minutes after isolation of the organism.
RAPID IDENTIFICATION
Turnaround time for this method is equivalent to a gram stain, but unlike a gram stain it provides definitive identification (ID) of the microorganism with over 98% certainty. The accuracy of this methodology is comparable to nucleic acid sequencing, but it is more cost effective and easily accessible, as it doesn’t require nucleic acid specific testing materials or kits and a longer time to results. If the organism requires specific resistance classification the report will indicate so, and a preliminary identification will be reported, with the organism and resistance reported later.
Included in this method’s compendium are organisms such as Candida auris, a deadly yeast, which is primarily only identifiable via this method. Historically, Candida auris has been transferred to a reference laboratory for identification, adding up to 48 hours to turnaround time.
Blood Cultures and Sepsis
The MBT Sensityper® test will also be available, and when used with the Bruker MALDI Biotyper® allows for identification of the organism directly from a positive blood culture bottle. When the bottle is flagged as positive, this method will allow us to provide a sample for identification on the MALDI in 15 to 20 minutes. This will effectively reduce the turnaround time for organism ID from a blood culture by up to 48 hours.
NICL Laboratories also has a PCR method available for a small menu of organisms, to provide antimicrobial susceptibility test results within a few hours of organism isolation and identification, and it can now be performed in a more selective manner, based upon the organism identified.
Antimicrobial Stewardship
Rapid organism identification from a culture bottle or a culture plate will provide for focused antimicrobial treatment and intervention. Coupled with NICL Laboratories annual MASTR™ report, the Bruker MALDI Biotyper® will assist the Infection Surveillance personnel in appropriate antimicrobial utilization. It will also provide for early determination of contamination, reducing the use of needless treatments.
Use of Broad Spectrum Antimicrobials and intravenous (IV) antimicrobials is very expensive. The use of PIC line and Midline catheters adds to the cost. The cost of use of Daptomycin over the period of a month can cost $9-10,000 and other drugs can cost as much as $33,000 for a one-month Medicare A stay. There is also risk attached to the use of these IV methods as they relate to nosocomial infections.
Use of this technology has an added benefit in that the microtiter wells on the plates used for organism ID can now be used to add a larger menu of antimicrobials for each organism identified, and for some antimicrobials, to provide a greater range of microtiters. BRUKER MALDI Biotyper® will help us to provide you with improved antimicrobial stewardship and patient outcomes.
Sepsis impact on Reimbursement
Hospital Acquired Conditions (HAC) such as sepsis, may impact a facility’s reimbursement. Every year the worst performing 25% are penalized by losing up to 1% of their Medicare payments. Targeted treatment may assist in reducing sepsis, and early successful treatment of other nosocomial infections, which will not only improve patient care and outcome, but it can also significantly impact the financial bottom line.
https://nicl.com/wp-content/uploads/2022/05/Bruker-mbt-sirius-with-user-bruker-md-web-thumbnail.jpeg511512NICL/wp-content/uploads/2022/04/nicl-logo-300x86.pngNICL2022-05-24 11:24:002022-09-23 14:40:18Antimicrobial Stewardship and the War on Sepsis
NOTE: Wear a gown, gloves, mask (N95 preferred), and eyewear when collecting these specimen.
1. Obtain specimen using only the mini-tip swab provided in the kit. Due to supply shortages, please use one swab per patient, please!
When collecting just a SARS CoV-2 sample, you may use an anterior nasal swab.
All other viral pathogen tests require a thin-tipped nasopharyngeal swab.
Swab Type
Collection Procedure
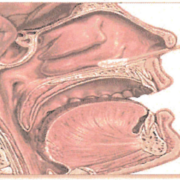
Nasopharyneal (N/P) swab
Has a very thin swab end; diameter of swab end is not much larger than swab handle
Push forward using gentle downward pressure to keep the swab on the floor of the nasal cavity until the tip reaches the posterior wall of the nasopharynx. Gently rub and roll the swab, and leave in place for several seconds to absorb fluid.*
It is not necessary to swab both sides if the swab is fully saturated from one side, but if both sides are collected, use a single swab on both the left and right nasal cavity.
A single swab may be used for SARS-CoV-2 and Influenza/RSV or Respiratory Viral Panel.
Anterior nasal swab
Swab end resembles a Q-tip. Do not attempt to collect a nasopharyngeal specimen using this type of swab.
Insert the swab at least one-half inch inside the nostril (naris) and firmly sample the nasal membrane by rotating the swab and leaving in place for 10 to 15 seconds.
Sample both nostrils with the same swab.
This type of swab can only be used for SARS-CoV-2 testing. It cannot be used for Influenza, RSV or other Respiratory Viral Pathogen testing.
*For a demonstration of N/P specimen collection please go to http://www.youtube.com/watch?v=DVJNWefmHjE (NEJM | Collection of Nasopharyngeal Specimens with the Swab Technique).
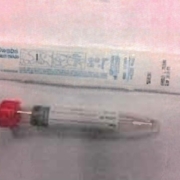
2. Break the shaft at the molded mark so that it can be placed in the tube without restricting the cap, and replace the cap tightly to prevent leakage and specimen rejection.
3. Label the vial with patient information (Name, DOB, collection date & time, specimen source and the test requested). Refrigerate it immediately.
4. Store the specimen refrigerated, and send it to the lab as soon as possible.
5. Complete the requisition. Indicate the swab type, and if the patient is symptomatic or if testing is for preoperative procedures. Race and ethnicity are also required by Health and Human Services. This is essential!
The above are M4RT media and other Viral transport media (check the label to see if the media should be kept refrigerated prior to collection). They are appropriate for Influenza, RSV, Respiratory Viral Panels and SARS-CoV-2 testing. NICL requires the use Viral transport media for its viral pathogens testing.
Outbreaks can happen in any facility, at any time. We all know that, but when it’s your facility, it can be very stressful. These are guidelines to help you when you have been told that there is an outbreak in your facility.
(1) Don’t panic!
(2) Give NICL Laboratories a call at (847) 509-9779. Speak to the Microbiology Supervisor, the Laboratory Technical Operations Manager, or your Customer Service Representative, or send them an email. NICL Laboratories is experienced with handling outbreaks and can help you and the Public Health Departments to gather the required information.
(3) Have the following information ready:
If IDPH (Illinois Department of Public Health) or your local health department has contacted the facility about an outbreak scenario, please provide the Contact Individual’s name to NICL so that we can secure the instructions for the particular outbreak.
Patient names and dates of birth
Case number assigned
(4) The Health Department may ask you to screen the other patients on the floor where there is an outbreak and/or to screen the employees that take care of the patients on that floor or unit.
(5) As soon as you let us know, we can create our Plan of Action, which may include:
Delivering more collection kits
Ordering more test kits/materials
Change of testing frequency
Add testing personnel
Coordinate specimens that need to be sent to IDPH, CCPH (Cook County Public Health), other health departments, or even the CDC (Centers for Disease Control)
Enterococci are part of normal gastrointestinal and genital tract flora.
Enterococci are gram positive cocci included in the Streptococci group D species; they are widely distributed in nature, animals and humans.
Among the 17 species currently recognized, E. faecalis and E. faecium are the most prominent in humans.
Infections that can be caused by enterococci include: UTI, bacteremia, wound, abdominal-pelvic infections and endocarditis.
Vancomycin is an important antibiotic used alone or in combination with other antibiotics for the treatment of serious infections caused by enterococci.
Resistance to Vancomycin
Vancomycin resistant enterococci (VRE) are multidrug resistant strains which present a serious difficulty in treating patients.
The resistance to vancomycin is induced by a genetic mechanism; the “VAN A gene” confers high-level resistance to vancomycin; it is plasmid mediated and can be transferred to other microorganisms such as Staphylococcus aureus. This may increase a possible emergence of VRSA (vancomycin resistant Staphylococcus aureus).
The patients can be “colonized” (carrying VRE without symptoms of infection), or “infected” (the presence of the VRE accompanied by clinical symptoms). They are both sources for nosocomial infection.
The most frequent sites for colonization are: stool, perineal, anus, axilla, umbilicus, wounds, foley catheter, and colostomy sites.
Epidemiology
Most infections and colonizations with VRE are attributed to the patient’s endogenous flora.
VRE can be spread by direct patient to patient contact or indirectly via hands of personnel, contaminated environmental surface or patient care equipment.
Prevention
Since vancomycin use has been reported consistently as a risk factor for colonization and infection with VRE, a restriction in the use of vancomycin should be imposed (see Hospital Infection Control Practices Advisory Committee recommendations).
It is strongly recommended for each facility to develop its own policies regarding the prevention and control of nosocomial transmission of VRE (isolation, culture survey, education program) according to the Hospital Infection Control Practices Advisory Committee (a copy is available from NICL).
Previously known as Flavobacterium meningosepticum, and more recently as Chryseobacterium meningosepticum, Elizabethkingia meningoseptica is a gram-negative bacterium found in soil and water. Although it is rarely isolated from clinical specimens, this organism is resistant to several classes of antimicrobials and is capable of causing infection in blood, cerebrospinal fluid, skin and soft tissue, the respiratory system, and other body sites. Nosocomial transmission of E. meningoseptica among immunocompromised adults in intensive care units has been reported. Further, long-term acute care hospitals with mechanically ventilated patients could serve as an important transmission setting for E. meningoseptica. This multidrug-resistant bacterium could pose additional risk when patients are transferred between long-term acute care facilities and other hospitals.
Please articulate and reinforce your established policies of infection control: handwashing and disinfection practices, isolation policies, the use of gowns and gloves, the proper disposal of body fluids and body fluid– contaminated items, and the use of sterile water for cleaning of respiratory equipment and any other devices that come into contact with mucous membranes or nonintact skin of patients. Additionally, adherence to the current CDC guidelines for prevention of Ventilator-Associated Pneumonia (VAP) is important for reducing these types of infections in the long-term acute care facility.
References:
Weaver, KN et al. Acute Emergence of Elizabethkingia meningoseptica Infection among Mechanically Ventilated Patients in a Long-Term Acute Care Facility. Infection Control and Hospital Epidemiology 2010, Vol. 31 (No. 1), pp. 54-58.
Walkey, AJ et al. Epidemiology of Ventilator-Associated Pneumonia in a Long-Term Acute Care Hospital. Infection Control and Hospital Epidemiology 2009, Vol. 30 (No. 4), pp 319-324.
Tablan OC, et al.; Centers for Disease Control and Prevention (CDC); Healthcare Infection Control Practices Advisory Committee. Guidelines for preventing health-care–associated pneumonia, 2003: recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR Recomm Rep 2004; 53(RR-3):1-36.
3/5/2020 NICL Laboratories, Ltd All Rights Reserved
NICL Laboratories will be providing new rapid molecular tests to aid in diagnosis of blood stream infections which could lead to sepsis. These new tests, called the Verigene® Blood Culture Nucleic Acid BC-GP or BC-GN, are for detection and identification of gram positive and gram negative organisms, respectively. These tests are also capable of detection of drug resistance markers. The test(s) will be automatically performed when a blood culture becomes positive.
Once a blood culture has been shown to be positive, a gram stain is performed to determine whether the organism is gram positive or gram negative, or if both are present. A sample is then submitted to the Verigene system for BC-GP (Gram Positive) or BC-GN (Gram Negative) organism identification. The results are available in approximately 3 hours. This will reduce the time for identification of the organism and resistance markers for 90% of organisms by nearly two days. The lists below indicate the organisms and resistance markers that can be detected.
Studies have shown that delayed administration of appropriate antibiotics is associated with a decrease in survival rate for each hour that the appropriate antimicrobial treatment is delayed*1. Rapid molecular testing of blood cultures has been shown to reduce this time and is associated with significant institutional cost savings*2.
The laboratory will continue to provide complete susceptibility profiles for blood culture isolates using conventional culture methods, to identify organisms not detected by this method, differentiate mixed culture growth, and to associate antimicrobial resistance marker genes to a specific organism.
*1.Bauer et al.2010. Clin Infect Dis, 51:1074-80
*2.Ly et al. 2008. Clin Risk Manag, 4:637-40
Bacterial Genera, Species and Resistance Markers
GRAM POSITIVE ORGANISMS
Organisms
Staphylococcus spp
Staphylococcus aureus
Staphulococcus epidermidis
Stahylococcus lugdunensis
Streptococcus spp
Streptococcus pneumonia
Streptococcus pyogenes
Streptococcus agalactiae
Streptococcus anginosus group
Enterococcus faecalis
Enterococcus faecium
Listeria spp
Resistance Markers
mecA gene, conferring methicillin resistance
vanA and vanB genes, conferring vancomycin resistance
GRAM NEGATIVE ORGANISMS
Organisms
Acinetobacter spp
Citrobacter spp
Enterobacter spp
Proteus spp
Escherichia coli
Klebsiella pneumonia
Klebsiella oxytoca
Pseudomonas aeruginosa
Resistance Markers
CTX-M (blaCTX-M)
KPC (blaKPC)
NDM (blaNDM)
VIM (blaVIM)
IMP (blaIMP)
OXA (blaOXA)
9/8/2017 NICL Laboratories, Ltd All Rights Reserved
Endocervical specimen collected on Aptima Unisex Swab submitted in transport tube. NOTE: Prior to female endocervical specimen collection, excess mucus must be removed with white cleaning swab provided in unisex swab collection kit. Discard white cleaning swab.
MALE:
Urethral swab collected on Aptima Unisex Swab submitted in transport tube. Discard white cleaning swab.
The patient should not have urinated for at least one hour prior to specimen collection.
Collect first 20 – 30 ml of voided urine (not midstream) in sterile, plastic preservative-free container. Minimum volume is 20ml. Maximum volume 60ml (NOTE: collection of larger volumes may result in dilution which may, in turn, reduce test sensitivity).
Transfer approximately 2 ml of urine into the Aptima Urine Specimen transport tube using the disposable pipette provided. Ensure fluid level is between the black lines on the urine specimen transport tube label. Do not overfill or underfill (testing will not be performed if the urine fluid level is not in between the two black lines on the transport tube). Urine specimens must be transferred into the Aptima Urine Specimen transport tube within 24 hours of collection and before being tested.
NOTE: Neisseria gonorrhoeae and chlamydia by nucleic acid amplification and trichomonas vaginalis naa testing are performed on the same Aptima tube and urine replicates are not required. The unisex swab cannot be used for testing males for trichomonas vaginalis. Please submit the urine swab.
NOTE: If other urine tests are requested, they must be submitted in separate plastic containers according to their individual requirements.
9/3/2019 NICL Laboratories, Ltd All Rights Reserved
NICL Laboratories is pleased to add Procalcitonin to our in-house esoteric testing menu. This test will be available seven (7) days per week.
Procalcitonin (PCT) is the precursor to calcitonin, and a specific marker for detection of severe bacterial infection and sepsis. Noninfectious inflammations need to be extremely severe for an increase in PCT to occur, making it a better indicator for sepsis than other inflammatory markers, such as cytokines, acute phase reactants, and interleukins. The elevations of PCT are also more sustained than most other markers and will also occur in neutropenic patients. This will reduce false negative results.
PCT begins to rise 2 to 4 hours after onset of severe infection or sepsis and peaks in 12-24 hours. The rise also parallels the severity of the infection/inflammation, as higher levels are found in the more severe infections, and the levels will fall as the inflammation subsides. PCT has a half life of 24-35 hours, making serial testing a useful tool for monitoring the patient’s inflammation or response to therapeutics. As PCT levels will decline as the inflammation subsides, it is also useful for identification of a secondary infection. If serial testing is indicated, the same sample type and testing location are recommended.
It should be noted that the sensitivity and specificity of PCT for sepsis ranges from 60% to 100%, and heterophile antibodies may interfere with all immunometric assays of this sort.
Interpretations
In adults, PCT levels less than 0.5 ng/mL represent a low risk of severe sepsis or septic shock, but cannot exclude local infection or systemic infection in early stages of less than 6 hours.
PCT levels between 0.2 and 2.0 ng/mL do not exclude an infection, because localized infections without systemic signs may be seen in these situations.
PCT levels greater than 2.0 ng/mL are highly suggestive of system bacterial infection or sepsis, or a very severe localized infection such as pneumonia, meningitis, or peritonitis.
PCT can also rise in non-infectious situations, such as major burns, severe trauma, acute multi-organ failure or with major abdominal surgery or cardiothoracic surgery, or prolonged or cardiogenic shock, but will generally begin to fall in 24 to 48 hours in these situations.
Autoimmune diseases, chronic inflammation, viral infections, and mild localized infections rarely lead to levels greater than 0.5 ng/mL.
Renal failure or insufficiency may also influence PCT values, and may confound diagnosis when present.
PCT can also be used to differentiate a viral from a bacterial infection.
If there is any disagreement between the laboratory results and the clinical signs, additional testing may be necessary.
5/30/2018 NICL Laboratories, Ltd All Rights Reserved
https://nicl.com/wp-content/uploads/2022/04/nicl-lab-bg.jpg10001500NICL/wp-content/uploads/2022/04/nicl-logo-300x86.pngNICL2018-05-30 11:44:002022-09-14 11:54:38Procalcitonin – for Detection of Severe Infection and Sepsis